Gastric sleeve surgery overview
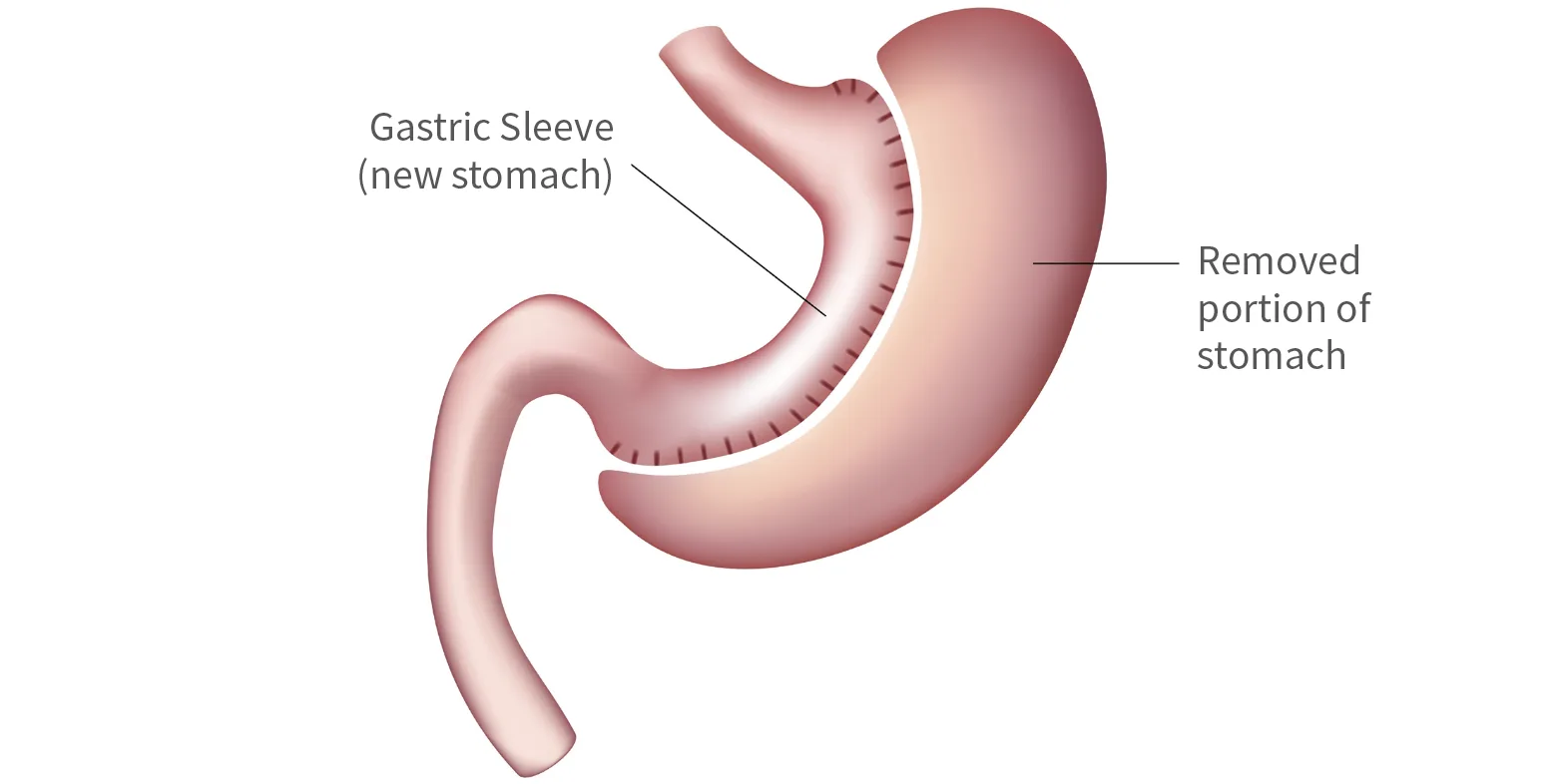
Gastric sleeve surgery reshapes the stomach, changing it from a large sac to a narrow tube. About 80% of the stomach is removed using keyhole (laparoscopic) surgery. With a smaller stomach, you feel full sooner and eat less. The surgery also lowers certain hormones that cause hunger, making it easier to manage your appetite.
Aside from these changes, your stomach continues to digest calories and absorb nutrients much like it did before.
A newer, safer approach
Gastric sleeve surgery has evolved from earlier procedures used to treat obesity. One of these, called vertical banded gastroplasty or “stomach stapling”, was stopped because it often caused problems like blockages.
The most common weight loss surgery in New Zealand and worldwide
The gastric sleeve was developed as a result of the problems seen with older surgeries like stomach stapling. Unlike those procedures, the sleeve does not use a band or ring, and the way it is created makes long-term complications far less likely.
How the sleeve became a stand-alone procedure
Gastric sleeve surgery (also called laparoscopic sleeve gastrectomy) was first used as the first step of a two-part weight loss operation for people with a very high BMI (usually over 50). It helped reduce risk before moving on to more complex surgery such as a bypass.
Surgeons soon noticed that many patients lost a significant amount of weight with the sleeve alone and didn’t need a second procedure. In the last 10 years, gastric sleeve surgery has become the most common type of weight loss surgery in New Zealand and worldwide.
What to expect after surgery
After surgery, your stomach needs time to heal. You’ll begin with liquids, move to puréed foods, and then return to eating three small meals a day. Most patients find entrée-sized portions are enough to feel full and satisfied, helping them eat less without feeling deprived.
A safe, minimally invasive procedure
The gastric sleeve is performed using laparoscopic (keyhole) surgery. Your surgeon makes several small cuts instead of one large one. A gentle gas inflates the abdomen to create space, and a small camera with fine instruments is used to perform the procedure with precision.
- Less pain after surgery
- A shorter hospital stay
- Faster recovery
- Lower risk of wound infection or hernia
In rare cases, if keyhole surgery cannot be completed, your surgeon may switch to open surgery. This is only done if it is the safest option for you.
Improved health
Weight loss surgery, like the gastric sleeve, can improve many health problems caused by obesity. Diabetes, sleep apnoea, joint pain, high blood pressure, and high cholesterol often get much better or even disappear after surgery.
Long-term weight loss
Most patients lose 60–70% of their excess weight after gastric sleeve surgery, which is about one-third of their total body weight. The biggest weight loss happens in the first year, with more gradual loss over the next 6–12 months. Weight usually stabilises after this, with only minor regain in some cases.
Success is best when patients make healthy lifestyle changes. That’s why at Auckland Weight Loss Surgery you will receive 6 Dietitian consults free of charge post weight loss surgery to help ensure long-term results. The laparoscopic gastric sleeve is not a quick fix but a powerful tool that makes these changes easier to achieve.
